|
I appreciated the recent opportunity to write a reflection on a class regarding the anti-psychiatry movement, mad studies, and strategies of attrition. I found it very resonant to my thinking about the role of naturopathic medicine in health care. I welcome your feedback!  The concepts of anti-psychiatry and the attrition model resonated for me on two key levels. The first is the alignment between the criticism of psychiatry, and my criticism of the dominant medical paradigm in general. The second resonance is the way in which the attrition framework lends some shape to the process of dismantling a powerful system, whether monopolized medicalization or capitalism. Similar to those in the antipsychiatry movement and as a naturopathic doctor (ND), I think in systems, particularly as it relates to the complex dynamics of the human body and mind, and the way in which an individual adapts and responds to social and ecological influences (Schleich, 2016; Solomonian, Batson, et al, 2020). That psychiatry has monopolized the mental health field, and the reductionistic nature by which it has done so, is but one example of the way that most healing paradigms that don’t fit the biopharmaceutical model have been marginalized. There are many reasons why our Western “health” system has arrived here - rooted in capitalistic, objectivist, Eurocentric worldviews that place profit and linear logic at the forefront (Haynes, 2009; Ashcroft & Van Katwyk, 2016). Excessive medicalization has (in my opinion and experience) two main consequences. Individuals who do not meet the criteria (whether biologic or syndromic) for a pathology based on current “validated” processes and outcome measures, epitomized by the International Coding of Disease system (Surján, 1999), are told there is nothing wrong with them thus denied care under our “universal healthcare” system. On the other end of the spectrum are those who have their condition diagnosed or labelled, and are told that its management lies solely within the biomedical domain. Both are consequences of systemic dismissal and devaluing of other ways of knowing, and come with significant costs (Ashcroft & Van Katwyk, 2016). Only those with the resources to do so are able to access other healing approaches (including strategies of primary prevention) - this is a harm of omission, leaving some incompletely cared for and others uncared for altogether as the context of their condition is disregarded. Consumers of naturopathic medicine (and non-psychiatric mental health practitioners) tend to sit in the upper strata of income and education unless the individual practitioner deliberately chooses to create systems that allow for greater access (Tippens & Connelly, 2007). This denies choice in healthcare (Gostin, Hodge, et al, 2003), and is a contributor to the complex mechanisms by which poverty and class constructs predict poor health (Stewart, Reutter, et al, 2005). Those who are told the only approach to disease management is pharmaceutical or surgical (or other barbaric treatments) may suffer from unmitigated adverse effects, especially if a practitioner is only concerned with a “disease-oriented” as opposed to a “patient-oriented” outcome (Sacristán, 2013). During the class, I was somewhat concerned with the response to my question about helping consumers become familiar with a counter-hegemonic paradigm, one that integrates context. The response seemed to focus on strategies of discouraging a pharmaceutical approach altogether. Although I understand the bias of the respondent, it felt incomplete. Certainly there are many potential harms associated with medicalization, whether stigmatization, physiologic adverse effects, masking of root causes, etc. However, in my personal and professional experience, pharmaceutical approaches are often helpful to enable and empower individuals to face and address the circumstances in which they have developed dysfunction or distress or “dis-ease.” As a result, I think I align more with “critical psychiatry” as opposed to anti-psychiatry. Whether treating cancer, symptoms of depression, or diabetes, an integrative approach based on holistic thinking, appropriate reliance on evidence, and genuinely informed consent means that ultimately nothing is completely off the table (figure 1). However, this does require that the power structures in our system be challenged to create space for and universal access to approaches other than an exclusively biomedical one. 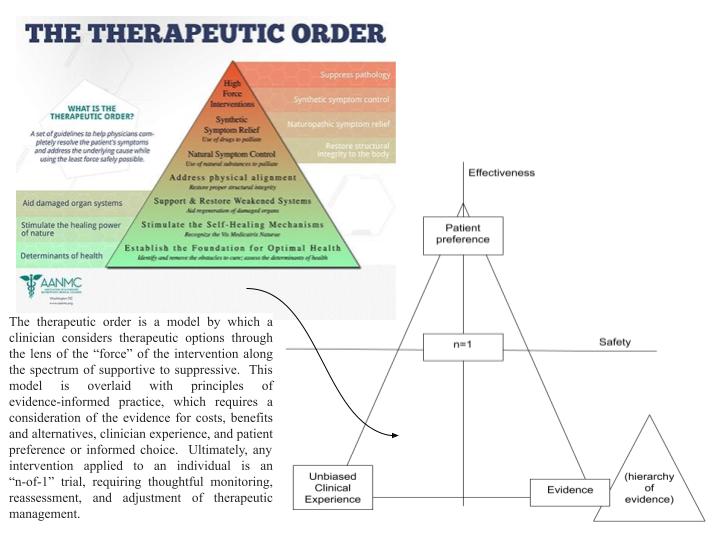 Figure 1: An Integrated Model for Evidence-Informed Practice (What is Naturopathic Medicine, 2020; Solomonian, 2019) Although I would not support abolishment of the biomedical approach completely, I do appreciate the merit of using the questions of the attrition model to guide strategic decision-making with respect to advocacy (Burstow, 2014):
1) If successful, will the actions or campaigns that we are contemplating move us closer to the long-range goal? 2) Are they likely to avoid improving or giving added legitimacy to the current system? 3) Do they avoid “widening” the net of the current system? For example, the Ontario Association of Naturopathic Doctors (OAND) is currently lobbying the Ministry of Health to expand our access to laboratory investigations (we have access to some but not all). The strategic leverage is that allowing NDs to order more labs saves the Ministry money through shifting the burden of payment to the private sector (OHIP does not cover the investigations that an ND orders). The association has argued that this “win” may elevate the role of NDs in the healthcare arena, chipping away at the dominance of the medical system over time, allowing for movement toward the greater goal of collaboration and integration. However, it seems to move us away from the goal of universal access to choice in healthcare by perpetuating a two-tier system. It also elevates the value of objectivism, legitimizing the biomedical approach. In a similar vein, efforts by the naturopathic and allied professions to elevate the legitimacy of so-called complementary and alternative medicine (CAM) serves to enable the dominant medical lobby to co-opt these approaches and “widen its net” while continuing to keep other paradigms at the margins (Baer & Coulter, 2008; Hollenberg & Muzzin, 2010). This is generally sought through the attempt to meet dominant standards of evidence in the form of RCTs and meta analyses, which - by design - control for “confounding” factors, deliberately disregarding the complexity of health and disease. The publication industry is vulnerable to bias at many levels, including the influence of Big Pharma (Brezis, 2008; Every‐Palmer & Howick, 2014). CAM therapies are not immune to the profitable siren call of the nutraceutical and “natural health product” industry (Haynes, 2009), which introduces another significant tension in the way these tools are applied - reductionistically or within a holistic paradigm (About naturopathy, n.d.). Ultimately, the effort to have CAM approaches legitimized by the dominant system only serves to reinforce the legitimacy of the biomedical paradigm. It also opens these approaches to co-optation; naturopathic medicine and other forms of complementary, integrative or alternative medicine are themselves guilty of colonization and appropriation (Waldron & Newton, 2012). Efforts to regulate professions, although ostensibly to protect the public, makes entry to them inaccessible to many, and removes practices from their context. This marginalizes and stigmatizes non-regulated traditional healers (Hollenberg & Muzzin, 2010), and has dire consequences when the disregard for non-Eurocentric epistemologies in which these paradigms are rooted threaten Planetary Health overall (Harawira, 1999; Solomonian, Batson, et al, 2020). If the Ministry of Health and Big Pharma are motivated by financial incentives, and the medical lobby is convinced by so-called high quality evidence, it is difficult to know how to move forward without buying into these problematic systems. “Whole-systems” research may achieve acceptable standards of evidence, and if paired with a cost-benefit analysis may interest those that manage the budget. Fortunately, the naturopathic profession is starting to produce this kind of research (Myers & Vigar, 2019). Engaging consumers - both those who do utilize other approaches, and those who would want to if they could access it - may be a way to build a base of support that could influence legislators through qualitative data and narratives. Considering the leverage points, the end goal, and the ways in which strategic actions may ultimately move us toward or away from this goal overtime are useful touchstones to guide advocacy; we have a long way to go. References
0 Comments
Leave a Reply. |
Archives
January 2024
Categories
All
|
 RSS Feed
RSS Feed
